
Fluid Status
Case:
75 year old male arrives to the emergency department. Past medical history of HTN, DM, HLD, BPH and foley placement 2 weeks ago. Patient is septic and taken to the resus room. On presentation the patient is altered, hypotensive and tachycardic. Vitals are
HR 123
BP 80/40
RR 27
Temp 39.0 C
02: 92% on room air

This patient is one that we have all seen many times. For many reaching for an ultrasound will be one of the first steps they take. With an ultrasound you can assess cardiac function, look for signs of fluid overload in the lungs as well as assess volume status with the IVC. Conventional wisdom used to say that IVC measurements were useful for volume status, as thinking has evolved it has become more clear that looking at the IVC is more likely useful only at the extremes of either being totally collapsed or plethoric (reference). Also seeing how much respiratory variation there is could also help a physician get an idea about a patient’s volume status. As more research has been done it has been shown that the IVC often correlated well to CVP or central venous pressure. The problem is that the CVP has come under more scrutiny and has been shown to only be useful on the extreme ends of being high or low when looking at volume status (2)
When assessing the volume status there are a few questions one usually asks. “Is the patient fluid down?”, is the patient “Volume overloaded?” A better clinical question that is more focused in these scenarios is actually “is the patient fluid responsive”, it has been shown that only around 50% of septic patients will respond to fluid (3) . Knowing this early may lead to the decision to use early pressors instead of repeat boluses which can have a negative effect on the patient.
The dynamic measurement called the Carotid flow time might be one tool a doctor can use to measure fluid responsiveness. The idea behind the measurement is that the carotid flow time is measured before and after a passive leg raise. The leg raise can be seen as a temporary bolus into the cardiovascular system. If the carotid flow time increases with the passive bolus that tells you that a patient has not yet plateaued on the frank starling curve and that the patient is able to increase cardiac output in response to increased preload.
Here are the steps to take carotid flow measurements

(a) First find the common carotid artery in the transverse plane to ensure you are over the target vessel.
(b) Next rotate the probe into the longitudinal axis to get the view needed for the measurements

Slide up the vessel until you see the carotid bulb (that is the slightly wider portion seen on the left side of the carotid in the above image) Usually found 2-3 cm was below the bifurcation of the CCA into the external and internal carotid arteries

The measurements we are taking are done just distal to the carotid bulb. Change the US machine into the pulse wave doppler mode
Place the carotid pulse wave gate in the middle of the vessel, then set the “correction angle” of the pulse wave measurement so that the green line is parallel to the the carotid artery. Note the red angle in the image at 89 degrees
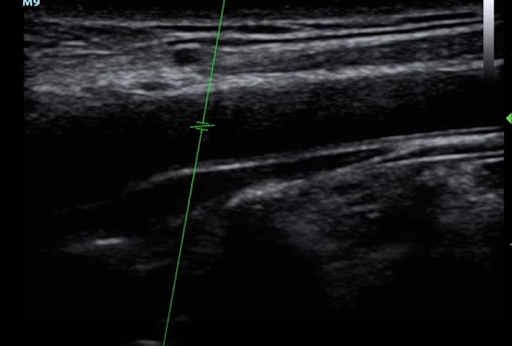
The angle between the “gate” and the steering line needs to be less than 60 degrees. The machine will tell you the angle and you may have to adjust the steering line to achieve an angle under 60 degrees

Turn on the pulse wave doppler, you will get the image above. The carotid flow time is measured with the formula ‘Systole time/ square root (cycle time). Note from above how the steering line was adjusted and the angle between the gate and steering line is now 52 degrees. Under 60 degrees now.

First find where systole starts and then locate the dicrotic notch as seen by the two blue arrows respectively in the images below. Systolic time is defined as the start of the systolic upstroke to the start of the dicrotic notch when the valves close. The cycle time is defined as the the time between two systolic upstrokes

Systolic time (0.34 seconds in this example)

Cycle time (0.69 seconds in this example)
Plugging these numbers into our formula of (systolic time/ square root of (cycle) time leads to a carotid flow time of 409mseconds. In one study fluid responsiveness was defined as an increase in the carotid flow time of 10% with a passive leg raise. In this study the sensitivity of the findings was %68 with a specificity of 96%. (4) The passive leg raise itself was defined as a the legs supported by a wedge at 45 degrees of elevation for 3 minutes. As this is a fairly new area of study in Ultrasound there are very few or no studies to be found comparing PLR vs an actual fluid bolus.
Although the carotid flow time is still experimental and under investigation it is a quick and easy measurement. Numerous factors such as if the patient is on mechanical ventilation, on inotropic agents and other factors can affect this measurement.
There is some evidence that a different measurement taken in this same view called the CBF or carotid blood flow is a more accurate measure of fluid responsiveness. (5) This measurement is more complicated and for those interested the formula for CBF is blood flow = π × (carotid diameter)2/4 × VTI × heart rate, where VTI indicates velocity time integral. The VTI is the tracing ot the cardiac cycle on the pulsewave and some machines can calculate this for you.
In summary carotid doppler is an up and coming area under research and measurements are easy to take after a bit of practice. It is probably not smart to hang your hat on any of these measurements but if you happen to think the patient is volume down clinically, the IVC is collapsible, the carotid blood flow and carotid flow time all increase with a passive leg raise you may have more information on the fluid responsiveness of your patient. As always nothing beats clinical judgement and these tools are all adjuncts to help with decision making.
References
Furtado S, Reis L. Inferior vena cava evaluation in fluid therapy decision making in intensive care: practical implications. Avaliação da veia cava inferior na decisão de fluidoterapia em cuidados intensivos: implicações práticas. Rev Bras Ter Intensiva. 2019;31(2):240-247. Published 2019 Jun 27. doi:10.5935/0103-507X.20190039
De Backer D, Vincent JL. Should we measure the central venous pressure to guide fluid management? Ten answers to 10 questions. Crit Care. 2018;22(1):43. Published 2018 Feb 23. doi:10.1186/s13054-018-1959-3
Douglas IS, Alapat PM, Corl KA, et al. Fluid Response Evaluation in Sepsis Hypotension and Shock: A Randomized Clinical Trial. Chest. 2020;158(4):1431-1445. doi:10.1016/j.chest.2020.04.025
MGH Ultrasound : Carotid ultrasound for volume responsiveness assessment (helpful images for steps taken from video)
Marik PE, Levitov A, Young A, et al. The use of bioreactance and carotid doppler to determine volume responsiveness and blood flow redistribution following passive leg raising in hemodynamically unstable patients. Chest. 2013;143:364–70.