
Flexor Tenosynovitis
Written by: Jing Jing Gong, MD; Edited by: Tim Khowong, MD
Introduction:
Pyogenic flexor tenosynovitis is an infection of the synovial sheath that surrounds the flexor tendon associated with penetrating trauma. As the flexor sheaths closely adjoin the deep spaces of the hand, this infection can easily spread quickly. Thus, flexor tenosynovitis is a surgical emergency. It accounts for 2.5-9.4% of all hand infections. Staph aureus accounts for 40-75% of all infections that cause this condition. Common risk factors include patients who suffer from diabetes mellitus, have history of IV drug abuse, or those who are immunocompromised.

Physical Exam:
Flexor tenosynovitis is a clinical diagnosis based on four physical exam signs collectively known as the Kanavel signs:
Fusiform swelling to the affected digit
Digit held in passive flexion at rest
Tenderness with percussion and/or palpation of flexor sheath
Pain with passive extension of the affected digit

Emergency Department Workup:
Basic laboratory workup in suspected tenosynovitis should include CBC and ESR to assess for leukocytosis and inflammatory marker elevations, which may or may not be present.
Imaging is not required for diagnosis of tenosynovitis, however X-rays may help to assess if there are foreign bodies or traumatic fractures present.
Point-of-care ultrasound in the emergency room may also assist in diagnosis of tenosynovitis. The patient’s hand can be fully immersed in water while a high-frequency linear transducer is used to visualize the affected digit. Concerning findings include peritendinous effusion (see figures) on the transverse or longitudinal views, or thickening of the tendon sheath visualized on ultrasound. The contralateral hand can be used as a control to account for any anatomy variability.
A prospective study in 2018 by Jardin et al identified 57 patients who had suspected flexor tenosynovitis and found that ultrasound demonstrated 94% sensitivity in diagnosis of flexor tenosynovitis.
Management:
The hand surgery team should be consulted emergently by ED providers. Empiric IV antibiotics should also be initiated, including vancomycin for MRSA and strep coverage, and ampicillin/sulbactam, or cefoxitin, or piperacillin/tazobactam for broad spectrum coverage. In patients who have a history of diabetes, pseudomonal coverage must be provided. In patients who have had marine exposure, consider adding a fluoroquinolone, or sulfamethoxazole/trimethoprim or doxycycline. IV antibiotics may suffice for patients who arrive with early presentation. These patients may also be offered splinting for comfort and immobilization If the patient demonstrates clinical improvement in 24 hours, no surgery is required. However, this is very rare. Most patients will require irrigation and washout in the OR. Even with appropriate treatment, complications of flexor tenosynovitis include subsequent stiffness, tendon or ligament pulley rupture, possible soft tissue infection due to adequate source control, loss of soft tissue, or even osteomyelitis.
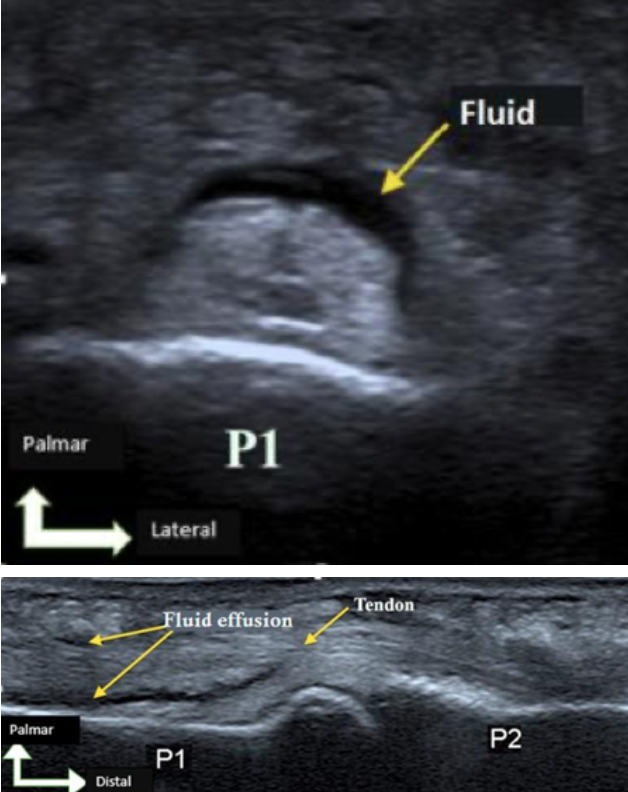
US findings in Flexor Tenosynovitis
References:
Donaldson, R, Alyssa M, Young N, Zonnoor B, Tan T, Rakofsky J, Holtz M, Arndt J, Swartz J, Ostermayer D. 2021. Flexor tenosynovitis. WikEM. Accessed on March 3, 2023. https://wikem.org/wiki/Flexor_tenosynovitis
Dyer K, Hussain A, Giladi A. Flexor tenosynovitis, 2019. NU EM Blog. Accessed on March 3, 2023. https://www.nuemblog.com/blog/flexor-tenosynovitis
Ghafoor N, Lema F, Yu C. Ultrasound probe: POCUS for flexor tenosynovitis. EMDocs. December 8, 2020. Accessed on March 3, 2023. http://www.emdocs.net/ultrasound-probe-pocus-for-flexor-tenosynovitis/
Jardin E, Delord M, Aubry S, Loisel F, Obert L. Usefulness of ultrasound for the diagnosis of pyogenic flexor tenosynovitis: A prospective single-center study of 57 cases. Hand Surg Rehabil. 2018;37(2):95-98. doi:10.1016/j.hansur.2017.12.004
Prats M. Flexor tenosynovitis. Ultrasound GEL Podcast, 2018. Accessed on March 3, 2023. https://www.ultrasoundgel.org/posts/q08ayJgg3rmHtiQgs9n82w
Scully EP, Earp BE, Miller AL, Loscalzo J. Just a Cut. New England Journal of Medicine, 2016; 375: 1780-1786. DOI: 10.1056/NEJMcps1512793
Yoon R. Pyogenic flexor tenosynovitis. Ortho Bullets, 2022. Accessed on March 3, 2023. https://www.orthobullets.com/hand/6105/pyogenic-flexor-tenosynovitis