
Humeral Shaft Fracture
Written by Luke Lin, MD
Edited by Victor Huang, MD, CAQ-SM
Case: A 80-year-old male with is brought in by EMS with severe right arm pain after he tripped and fell down 2 steps. He reports injuring his right upper arm. The exam reveals deformity and swelling to his right upper arm. Neurovascular examination is intact.
What is the diagnosis, typical mechanism of injury, expected physical exam findings, appropriate imaging modalities, and management plan?
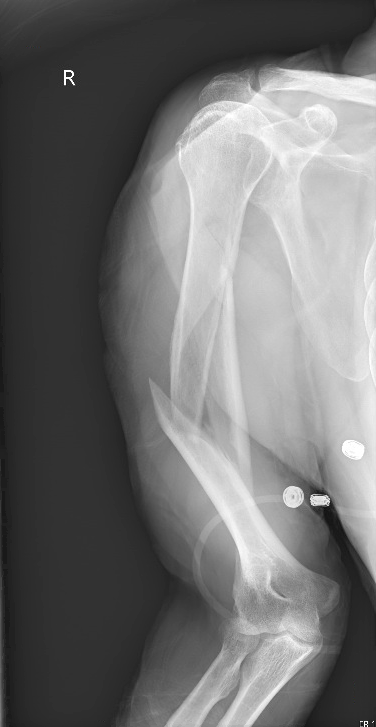
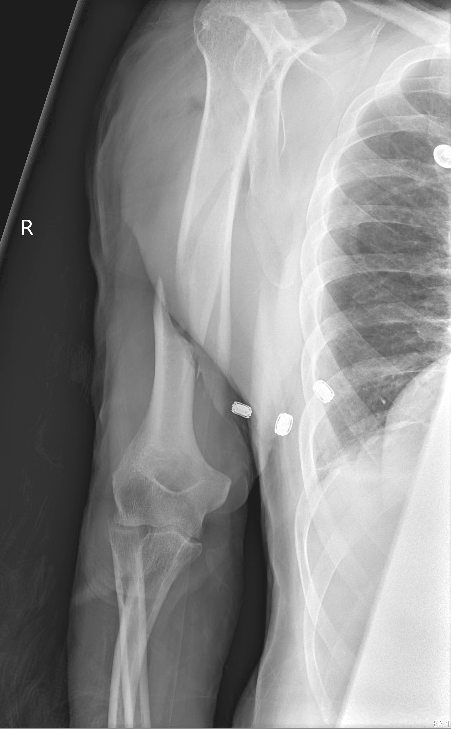
Figure 1. AP and lateral views of the right humerus that demonstrate a comminuted and displaced fracture of the humeral shaft with significant varus angulation. Author’s own images.
Introduction
Humeral shaft fractures are common and account for 3% of all fractures. Even though the majority of these fractures are unstable, they typically do well with non-operative management [1,2].
Patients who sustain humeral shaft fractures fall under a bimodal age distribution. Most are either young patients with high-energy trauma with a or elderly, osteopenic patients with low-energy injuries [1]. The typical mechanisms of injury are a direct blow or a fall on outstretched arm [2-4].
![Figure: AO classification of humeral shaft fractures [10].](https://images.squarespace-cdn.com/content/v1/5bc94f5b9b7d1515843688af/1607052514123-19ZT1IO6FATH32TY5V7H/humeral+shaft+fx+types.png)
Figure: AO classification of humeral shaft fractures [10].
Clinical Evaluation
Patients often present with a deformity of the upper arm that is shortened and displacement is dependent on the level of the fracture relative to the muscle attachments of the pectoralis major and the deltoid (see figure 2). Complications include acute compartment syndrome and radial nerve palsy. Therefore, it is important to conduct a thorough neurovascular exam [3,4].
![Figure 2: Displacement of humeral shaft fractures is dependent on the level of the fracture in relation to the muscle attachments of the pectoralis major and the deltoid [4].](https://images.squarespace-cdn.com/content/v1/5bc94f5b9b7d1515843688af/1607052049876-T02X1FHN8G1ACYX7KCF3/humerus+shaft+fracture+-+eiff+picture+copy.png)
Figure 2: Displacement of humeral shaft fractures is dependent on the level of the fracture in relation to the muscle attachments of the pectoralis major and the deltoid [4].
The radial nerve runs along the spiral groove of the humerus and is the most commonly injured nerve with humeral shaft fractures, seen in 11.8% of cases [5]. Assess for radial nerve deficits including loss of extension of the elbow, wrist and fingers, weakness of supination, and sensory loss in the radial distribution [3].

Figure: Radial nerve entrapment due to humeral shaft fracture. (https://www.mplsortho.com/conditions-treatments/ecategory/47/etopic/4e9a2e8d8583ef20c2f7a72ebfa65420)
Plain radiographs of the humerus in two orthogonal planes should be obtained. Also, the joints above and below should be assessed for possible imaging to evaluate for extension of the fracture and concomitant injuries shoulder dislocation and forearm fractures (floating elbow) [2,3].
Management
Humeral shaft fractures can be immobilized with a hanging arm cast or a coaptation splint (see Figure ). The splint will start from the axilla, wrap around the elbow which should be flexed to 90 degrees, and extend over the acromion process. Utilize a valgus mold to counter the typical varus displacement. Support the wrist with a collar and cuff sling, while keeping the elbow unsupported to provide traction [4,6,8].
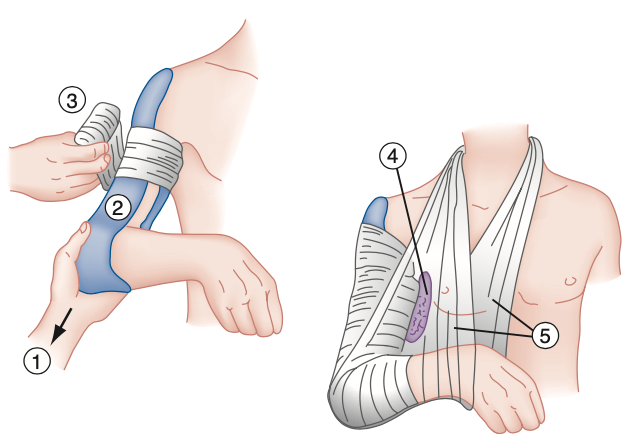
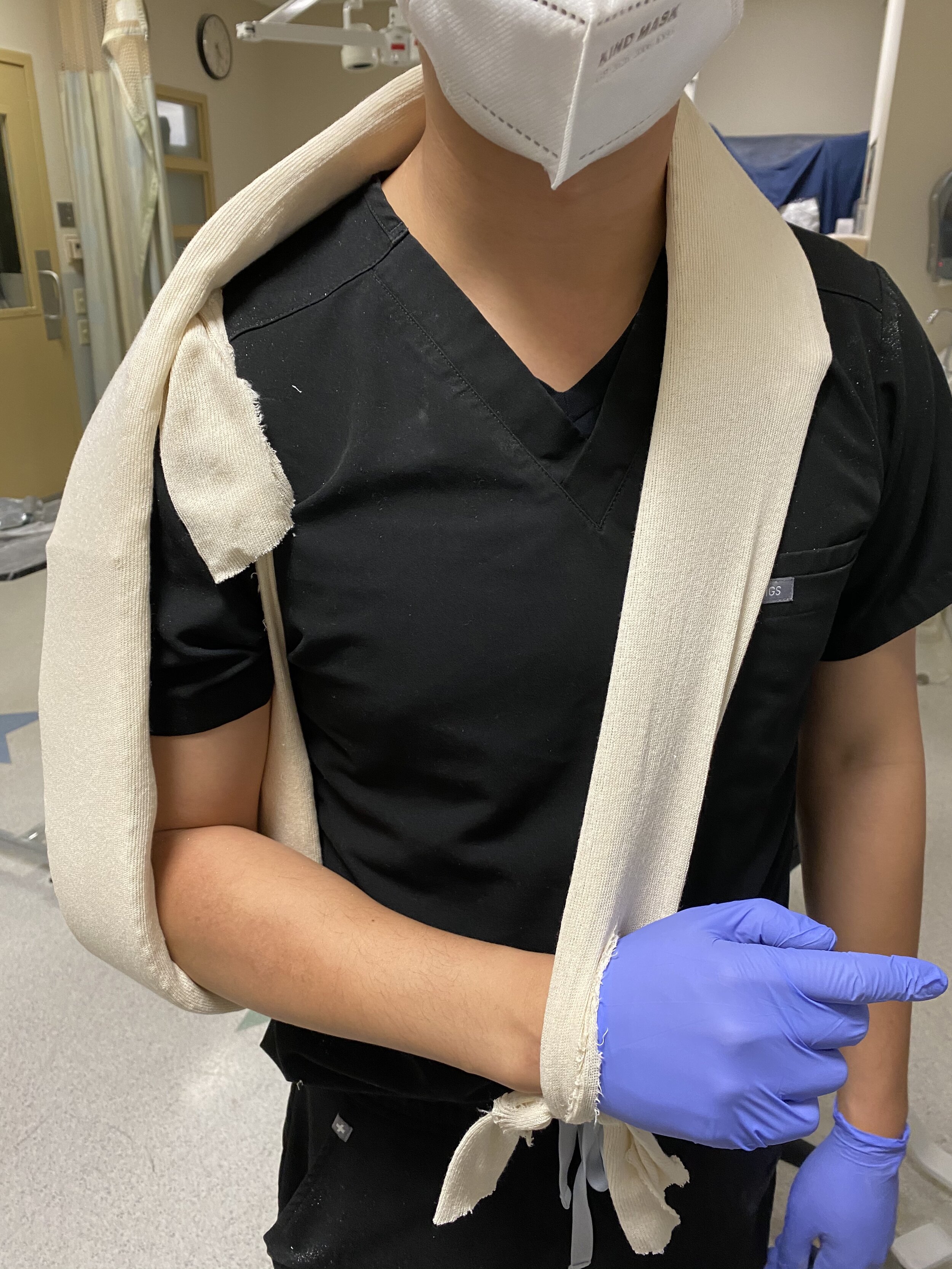

Figure: Coaptation splint [3]


Figure: Post-reduction radiographs of the right humerus after coaptation splint application. Author’s own images.
Non-operative management is the mainstay of treatment for the majority of cases, with acceptable healing in over 90% of patients as malunions with residual angulation can be well-tolerated due to the mobility of the shoulder and elbow [1-3]. The initial splint is replaced within 2 weeks with a Sarmiento (functional) brace that provides fracture stabilization through circumferential soft-tissue compression [1,4].
![Figure: Sarmiento (functional) brace [11]](https://images.squarespace-cdn.com/content/v1/5bc94f5b9b7d1515843688af/1607053735330-E3HXMJXXTDDJ2KAQD262/Schematic-image-of-a-Sarmiento-functional-brace-The-material-is-a-Thermoplastic.png)
Figure: Sarmiento (functional) brace [11]
Surgical intervention such as plate fixation and intramedullary nailing is indicated for open or comminuted fractures, vascular injury, brachial plexus injury, ipsilateral forearm fracture (floating elbow), and compartment syndrome [1,2,7].

Figure: Intramedullary nail (case courtesy of Dr Sajoscha Sorrentino, Radiopaedia.org, rID: 15644)
Meanwhile, if neurological deficits including radial nerve palsy are present, a NCS/EMG should be performed after 6 weeks to assess the extent of nerve damage, monitor recovery, and determine if surgical exploration of the nerve is necessary [1]. However, more than 80% of radial nerve injuries recover spontaneously [5].
Works Cited
Walker M, Palumbo B, Badman B, Brooks J, Van Gelderen J, Mighell M. Humeral shaft fractures: a review. J Shoulder Elb Surg. 2011;20(5):833-844. PMID: 21393016
Bounds EJ, Frane N, Kok SJ. Humeral Shaft Fractures. [Updated 2020 Aug 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448074/
Bookman K. Humerus and Elbow. In: Rosen’s Emergency Medicine: Concepts and Clinical Practice. 9th Ed. Elsevier; 2018:530-548.
Eiff MP, Hatch R. Humerus Fractures. In: Fracture Management for Primary Care. 3rd Ed. Elsevier; 2018:154-174.
Korompilias A V., Lykissas MG, Kostas-Agnantis IP, Vekris MD, Soucacos PN, Beris AE. Approach to radial nerve palsy caused by humerus shaft fracture: Is primary exploration necessary? Injury. 2013;44(3):323-326. PMID: 23352153
Zehms CT, Balsamo L, Dunbar R. Coaptation splinting for humeral shaft fractures in adults and children: a modified method. Am J Orthop. 2006;35(10):452-454. PMID: 17131733
Ouyang H, Xiong J, Xiang P, Cui Z, Chen L, Yu B. Plate versus intramedullary nail fixation in the treatment of humeral shaft fractures: an updated meta-analysis. J Shoulder Elb Surg. 2013;22(3):387-395. PMID: 22947239
Shantharam SS. Tips of the trade #41: Modified coaptation splint for humeral shaft fractures. Orthop Rev. 1991;20(11):1033-1039. PMID: 1749659
Venouziou AI, Dailiana ZH, Varitimidis SE, Hantes ME, Gougoulias NE, Malizos KN. Radial nerve palsy associated with humeral shaft fracture. Is the energy of trauma a prognostic factor? Injury. 2011;42(11):1289-1293. PMID: 21353219
Strohm P, et al. Humerus shaft fractures - where are we today? Acta chirurgiae orthopaedicae et traumatologiae Cechoslovaca, 2011;78(3):185-9.
Mader K, Mader S, Berntsson P. The Diaphysis: Nonsurgical Treatment. Simple and Complex Fractures of the Humerus. 2015.