
Ortho Case: Knee Laceration
Author: Victor Huang, MD, Peer-review and editing: Tabitha Ford, Gabby Ahlzadeh, Will Denq
Case: 20-year-old male presented with a laceration over the superomedial aspect of the right knee after being struck by a car.

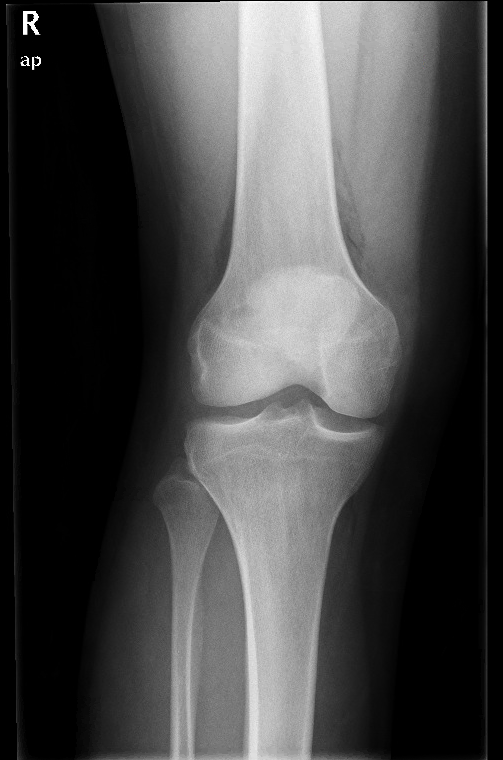
Figure 1a. Image prompt. AP view of knee. Author’s own images.

Figure 2a. Lateral view of knee.
What is the diagnosis?
What are the typical mechanisms of injury?
What is the diagnostic approach?
What is the management in the ED?
What is the definitive management of this injury?
See below for answers!
1. What is the diagnosis?
Traumatic arthrotomy of the knee. The plain radiographs demonstrate air in the suprapatellar compartment with a small joint effusion.
PEARL: Wounds that are located near joints should always be evaluated for joint involvement.1-4 The knee is the most commonly affected joint, comprising 51% to 91% of injuries.1,2 It is essential to diagnose this injury because it is a significant risk for septic arthritis, developing in up to 11.8% of cases.1-3,5
2. What are the typical mechanisms of injury?
The majority are due to gunshot wounds (43%), motor vehicle accidents (20%), falls, and sharp objects.1,2,5
3. What is the diagnostic approach?
Inspect the wound for intra-articular contents including visible joint surface.1,2
Obtain a plain radiograph to assess for intra-articular air or foreign body.1-6 41% of cases are diagnosed by examination and radiographs.2
When there is still diagnostic uncertainty, CT is the next best diagnostic modality for traumatic arthrotomies, with 100% sensitivity and 100% specificity.2,5
The “saline load test” (SLT) is a procedure where sterile saline is injected into the joint at a site separate from the injury. If there is extravasation of fluid from the wound, the joint has been violated.1,4,5 Afterwards, the remaining saline should be aspirated.4 SLT can be 99% sensitive, but this would require injection of 175-194 mL into the knee.1,2,5,6 Furthermore, it is invasive, increases intra-articular pressure, and can cause significant discomfort.4 There may be a role for SLT when CT imaging is unavailable in the ED.5

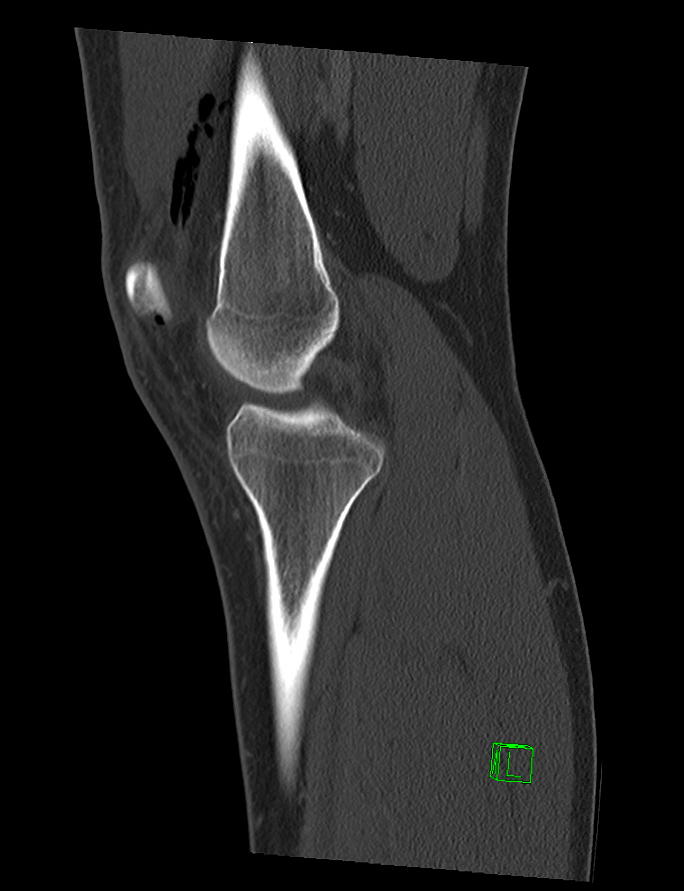
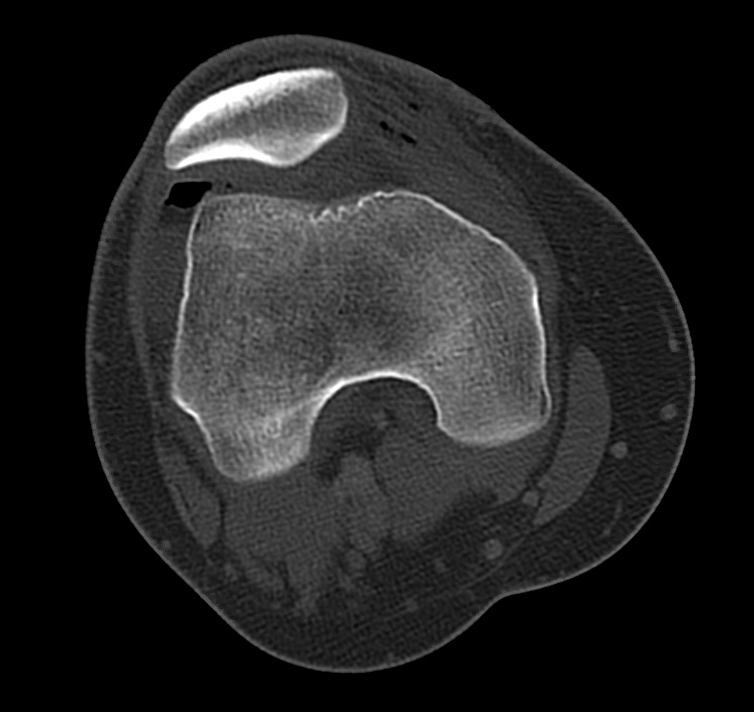
Figure 2. CT images of the right knee demonstrating intra-articular gas within the suprapatellar recess and the medial aspect of the patellofemoral compartment, as well as a mildly depressed impaction fracture of the medial femoral condyle. Author’s own images.
4. What is the management in the ED?
The patient should be given tetanus prophylaxis and antibiotics to cover streptococci and staphylococci, such as a cephalosporin.1-3,6,7 Cover the wound with moist sterile dressings and splint the joint in extension.2,4
5. What is the definitive management of this injury?
Orthopedic surgery should be immediately consulted. The patient should be admitted for urgent irrigation and debridement of the joint to remove contaminants, foreign bodies, bone fragments, and necrotic tissue.1,2,7 Open and arthroscopic approaches are both utilized. An open procedure may be preferred for large lacerations and contamination, or those with an associated fracture. Arthroscopy may be preferred for smaller lacerations with minimal soft-tissue injury.1,2
References
Nord RM, Quach T, Walsh M, Pereira D, Tejwani NC. Detection of traumatic arthrotomy of the knee using the saline solution load test. The Journal of Bone & Joint Surgery. 2009;91(1):66-70. doi: 10.2106/JBJS.G.01682.
Konda SR, Davidovitch RI, Egol KA. Open knee joint injuries: An evidence-based approach to management. Bulletin of the Hospital for Joint Diseases. 2014;72(1):61-69.
Roberts TD. Traumatic arthrotomy with pneumoarthrosis on plain radiograph of the knee. Western Journal of Emergency Medicine. 2016;17(2):184-185. doi: 10.5811/westjem.2015.12.29317.
Sanford SO. Joint arthrography. In Roberts et al. eds. Roberts & Hedges’ Clinical Procedures in Emergency Medicine. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014: 1092-1094.
Browning BB, Ventimiglia AV, Dixit A, Illical E, Urban WP, Jauregui JJ. Does the saline load test still have a role in the orthopaedic world? A systematic review of the literature. Acta Orthopaedica et Traumatologica Turcica. 2016;50(6):597-600. doi: 10.1016/j.aott.2016.01.004.
Bengtzen R. Knee injuries. In: Tintinalli JE, et al. eds. Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th ed. New York, NY: McGraw-Hill; http://accessmedicine.mhmedical.com/content.aspx?bookid=2353§ionid=222407442. Accessed January 13, 2020.
Smith WR, Stahel PF, Suzuki T, Gabrielle P. Musculoskeletal trauma surgery. In: Skinner HB, McMahon PJ. eds. Current Diagnosis & Treatment in Orthopedics, 5th ed. New York, NY: McGraw-Hill; 2014. http://accessmedicine.mhmedical.com/content.aspx?bookid=675§ionid=45451708. Accessed January 13, 2020.
Image from US Army Africa. Available at: https://www.flickr.com/photos/usarmyafrica/25161064891/in/album-72157662631748263/. Accessed February 19, 2020.
This post was shared with permission by the team from Wild Ortho Wednesdays. For more ortho pearls delivered straight to your email, you can click here to request to join the group! Log into your google account and provide your background information in order to access the link and be approved to join the listserv.