
"J" Day
Written By: Brian Smith, DO
A patient is brought in by EMS post cardiac arrest:
A 55-year-old man presents to the ED after being found by EMS laying on a park bench in PEA arrest. Chest compressions were initiated and epinephrine was given once, after which ROSC was obtained. He is pale-appearing and cool to touch but does have palpable radial and DP pulses. An ECG is obtained on arrival and shown below.

Question: Which of the following is indicated at this time?
A) TPA
B) Activate code STEMI
C) Calcium Gluconate IV
D) Warm IV Fluids
Answer: D) Warm IV Fluids
Given our clinical vignette and ECG changes, our patient most likely suffered a cardiac arrest due to hypothermia. Our patient was found to have a core body temperature of 30 C on arrival.
There are many ECG changes that can be seen in hypothermic patients, so let’s review them:
ECG Changes in Hypothermia:
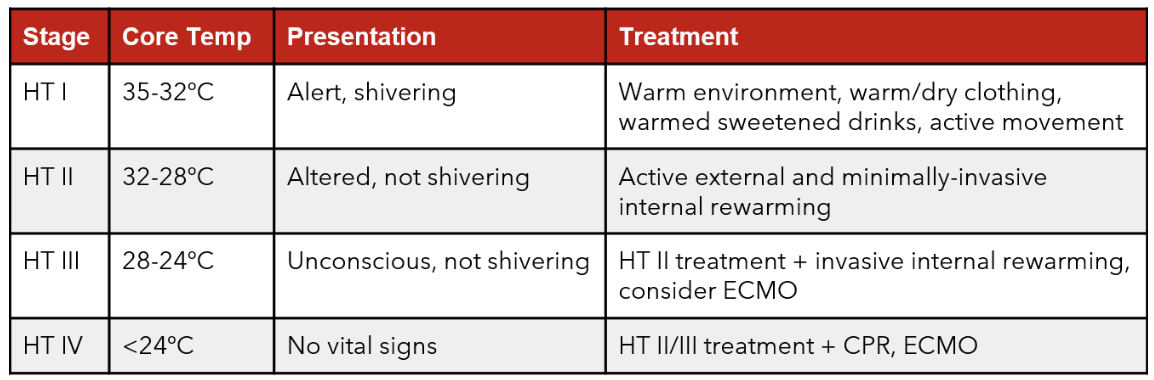
Stages of hypothermia. Source: https://www.tamingthesru.com/blog//air-care-series/accidental-hypothermia
Bradyarrythmias
Sinus Bradycardia
Atrial Fibrillation with Slow Ventricular Response
Junctional Bradycardia
AV block
Prolonged PR, QRS, and/or QT intervals
Shivering Artifact
Can be seen in mild hypothermia
Shivering stops when temperature reaches moderate hypothermia (30-32 C)
Osborn (J) Wave
Positive deflection at the J point (end of QRS complex) in the precordial and limb leads
Reciprocal Negative J point deflection in aVR and V1

Here is an ECG of a hypothermic patient. Can you point out the signs of hypothermia in the ECG?
Source: LITFL https://litfl.com/hypothermia-ecg-library/
Answer: Sinus bradycardia, shivering artifact, Osborn (J) wave
Looking back at our patient’s ECG, there are a few of these changes present:

Here we see Osborn (J) waves - upward deflection of J point in precordial leads - best seen in V4-V6, inferior leads, and lead I (blue asterisks) - with reciprocal negative deflection in aVR (red arrows)
The patient also has QTc prolongation, specifically due to prolonging of the ST segment (similar to hypocalcemia)
Let’s dive a bit deeper into J waves:
The size of the J wave is INVERSELY PROPORTIONAL to temperature.
In the image below we see a decreasing amplitude of the J wave with increasing temperature during the active rewarming process

Source: LITFL https://litfl.com/osborn-wave-j-wave-ecg-library/
While J waves are most commonly associated with hypothermia, there are many other causes:

Hypercalcemia
Acute MI
Takotsubo cardiomyopathy
Myocarditis
Brugada syndrome
Left ventricular hypertrophy
Benign early repolarization
Increased Intracranial pressure
Summary:
There are many ECG changes associated with hypothermia
The height of the Osborn (J) wave is inversely proportional to temperature
While most commonly associated with hypothermia, there are many other causes of Osborn (J) waves