
Analysis of Paralysis
Brian Smith, DO
You are working in the main ED
Your next patient is a 27-year-old otherwise healthy male who awoke with generalized weakness. He states he returned from a bachelor party in Mexico last night and woke up this morning unable to move his arms or legs. He reports that during his trip, his diet consisted mostly of “beer, chips, and salsa”. He also endorses multiple episodes of watery diarrhea x 2 days but denies any other complaints. He states this has never happened before.
His vitals are within normal limits.
On exam, you note ⅖ strength in hip flexion and extension and shoulder abduction. He has ⅗ strength in knee and elbow flexion and extension and ⅘ strength in ankles and wrists.
His ECG is shown below

Question: What test will clinch the diagnosis?
Before you scroll, look carefully at the ECG. There are 3 clues pointing to the cause of the patient’s symptoms!
Answer: Serum Potassium Level
This patient is presenting with Hypokalemic Periodic Paralysis. Before we discuss the pathology, lets first dive into the ECG changes suggestive of hypokalemia
Hypokalemia
The “Push-Pull Effect”: Comparing ECG changes associated with Hypokalemia with Hyperkalemia

Hypokalemic Periodic Paralysis:
Mechanism:
Autosomal dominant sodium channelopathy associated with young asian males
Potassium Shifts
Thyrotoxicosis
High carbohydrate diet (increased insulin release)
Potassium Losses (GI and/or renal)
History:
Strenuous Exercise
High carbohydrate/sodium intake
Sudden temperature change
Emotional stress
Attacks can last hours
Exam:
Hyporeflexia
Flaccid paralysis in proximal > distal extremities
Workup:
BMP and Serum magnesium level
Thyroid panel
ECG
Management:
Judicious K+ repletion
Consider magnesium
Consider propanolol (3 mg/kg PO)
Escpecially for thyrotoxicosis varient
Back to the Patient:
The patient’s serum K+ was 1.3. He was given PO and IV potassium supplementation as well as IV magnesium. he was Admitted to MICU for frequent neurochecks and close monitoring of potassium leves.
Made a full recovery and discharged the next day
Take Home Points:
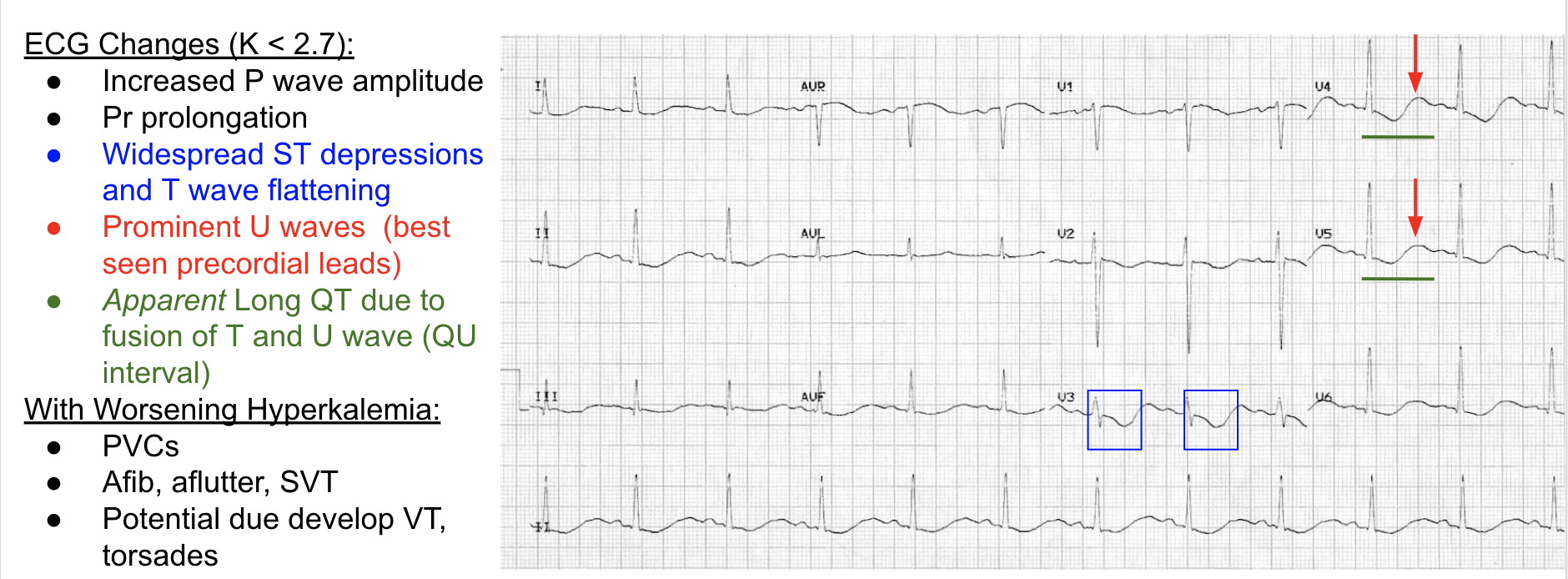
ECG changes with Hypokalemia:
Widespread ST depressions and T-wave flattening
Prominent U waves
Apparent long QT interval due to fusion of T and U wave.
Consider Hypokalemic Periodic Paralysis for patients with sudden onset flaccid paralysis

If you have trouble remembering risk factors for Hypokalemic Periodic Paralysis, think of a frat boy on spring break