
Serratus Anterior Block
Rib Fractures…Yeah Ultrasound Is Useful in That Situation As Well
Written by: Ashraf Hussain MD. Edited by: Jeff Greco MD
It’s a busy overnight shift in your already busy emergency room when at 3 am you hear overhead that a trauma is coming into the emergency room. You walk over and notice an 82-year-old woman who slipped and fell in the bathroom. She is alert and screaming in pain. You complete her primary survey and give her some fentanyl to complete the second. As you judiciously do her secondary survey you note anterolateral chest wall tenderness at the 4th to 7th ribs. The amazing resident that you are you complete your eFAST, see no pneumothorax or free fluid, and rush her to additional imaging. You find that she in fact has rib fractures on ribs 3-7. Luckily, she doesn’t have flail chest, but she is still in significant amount of pain. An hour passes by and she requires multiple doses of fentanyl and subsequently morphine. She remains in pain, but you don’t feel comfortable giving her any more narcotic pain medications. As you ponder about what in your armamentarium to use to control her pain in between pushing for the admission to the trauma team your attending suggests doing a serratus anterior block.
What is the serratus anterior block?
It is an ultrasound guided block that anesthetizes the lateral cutaneous intercostal nerves.
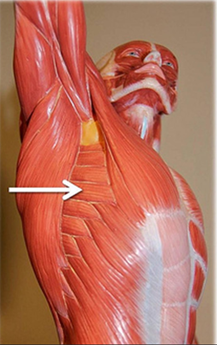
Anatomy
The chest wall is innervated by the lateral cutaneous intercostal nerves which branch off of the thoracic intercostal nerves. The lateral cutaneous nerves innervate the interior and exterior intercostal nerves as well as the serratus anterior. They lie superficial to the serratus anterior muscle. The serratus anterior muscle lies superficial to the ribs.
Materials

Obtain consent Extra person to help inject anesthetic Linear ultrasound probe Sterile probe cover Anesthetic: 15 mL ropivacaine 0.5% (5 mg/mL; maximum 3 mg/kg) and 15 mL normal saline placed in a 30 mL syringe 22 g blunt-tip block needle 36 inch tubing Chlorhexidine 25g needle for local skin wheal Lidocaine for skin wheal Lipid emulsion 20% for anesthetic systemic toxicity - 1.5 mL/kg bolus over 1 minute - Followed by 0.25 mL/kg/min for 20 min or until hemodynamic stability is achieved.
How to do
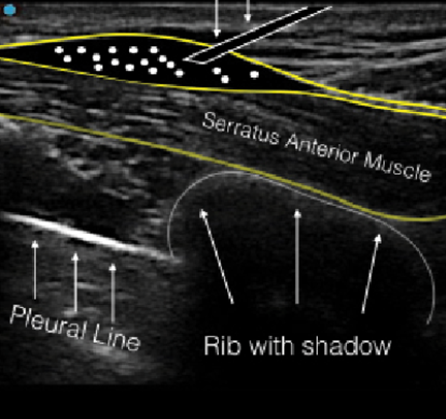
Place patient on cardiac and oxygen monitoring Perform time out Place patient in lateral decubitus position with unaffected side down Place probe with sterile probe cover at patients 4th or 5th rib mid axillary line with probe marker facing towards the patient’s nipple
Locate ribs with serratus anterior found superficial to ribs and latissimus dorsi muscle found laterally. The anterior fascial plane will lie superficial to the serratus anterior and deep to the latissimus dorsi
Clean over area Place probe back over area and using 25-gauge needle and using in plane technique create skin wheal over area Using the 22-gauge needle use in plane technique insert needle with needle in sight at all times. One you located fascial plane hydro dissect with 2-3mls of anesthetic. If in right location continue with injection of anesthesia into fascial plane Remove needle and place band-aid Reassess patient pain in 15 minutes

Evidence
Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Bianco. et. al. 2013
- Thirty minutes after injection the 4 volunteers reported numbness in dermatome T2-T9. Mean duration of anesthesia was 752 minutes for the intercostal muscles.
A randomized trial of serratus anterior plane block for analgesia after thoracoscopic surgery. Park et. al 2018
- SAFB block reduced fentanyl consumption, worst pain score reported in the first 24 hours after surgery vs patients who did not receive the SAFB
Ultrasound-Guided Serratus Anterior Plane Block Versus Thoracic Epidural Analgesia for Thoracotomy Pain. Khalil et. al. 2017
- 40 patients who had undergone a thoracotomy were randomly selected to receive a SAFB vs a thoracic epidural catheter for post-op pain control. Although the total dose of morphine consumption was unchanged in both groups, MAP was decreased in the epidural catheter group vs the SAFB group.
Bottomline: Ultrasound guided SAFB may be a great adjunct for pain control in patients with rib fractures. It is a relatively quick procedure once you identify the anatomy. Remember to reassess the pain and always have lipid emulsion at bedside.
References
1. Southgate SJ, Herbst MK. Ultrasound Guided Serratus Anterior Blocks. [Updated 2019 Mar 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538476/
2. https://www.acepnow.com/article/ultrasound-guided-serratus-anterior-plane-block-can-help- avoid-opioid-use-patients-rib-fractures/?singlepage=1
3. Blanco, R., et al. “Serratus Plane Block: a Novel Ultrasound-Guided Thoracic Wall Nerve Block.” Anaesthesia, vol. 68, no. 11, 2013, pp. 1107–1113., doi:10.1111/anae.12344.
4. Khalil, Asmaa Elsayed, et al. “Ultrasound-Guided Serratus Anterior Plane Block Versus Thoracic Epidural Analgesia for Thoracotomy Pain.” Journal of Cardiothoracic and Vascular Anesthesia, vol. 31, no. 1, 2017, pp. 152–158., doi:10.1053/j.jvca.2016.08.023.
5. Park, M. H., et al. “A Randomised Trial of Serratus Anterior Plane Block for Analgesia after Thoracoscopic Surgery.” Anaesthesia, vol. 73, no. 10, 2018, pp. 1260–1264., doi:10.1111/anae.14424.