
Resuscitative TEE: Taking Cardiac Ultrasound to the Next Level
Written by Kenny Chang, MD. Edited by Jeff Greco, MD.
Case:
A morbidly obese middle-aged male is brought in by EMS in cardiac arrest after collapsing at a local store across the street from your emergency department. Luckily, his witnessed downtime has been only approximately 5 minutes as the EMTs were on break at the store. Patient has been in PEA, with 1 dose of epinephrine given on the 2 pulse checks. As the ultrasound resident, you pull up with the cardiac probe trying to squeeze in all while your classmates and nurses are trying to put in an IO, placing defibrillator pads, and much more. You try to squeeze in during the pulse check but are unable to see a good subxiphoid view of the heart. The LUCAS device starts up again before you can try and get a parasternal long axis. Now... if only there was a more effective way of doing this?
Although the TEE (transesophageal echocardiogram) has not yet become a common standard of care during cardiac arrests unlike the TTE (transthoracic echocardiogram), it has been an even more superior tool in helping resuscitationists make clinical decisions during the stressful management of cardiac arrests.
Why the TEE?
Higher resolution images (not affected by patient’s body habitus, defibrillator pads, subcutaneous air, etc)
Can be used continuously without pausing compressions while monitoring for chest compression quality
TEE can be used to obtain views that are anatomically similar to those used in TTE views
Why not the TTE?
The only absolute contraindication would be for esophageal perforations or injuries.
Placement of a supraglottic airway would also preclude the use of TEE.
Clinical Pearls
The cardinal movements include advancing and withdrawing the probe, turning the probe, ante-flexing or retro-flexing, rotating (multiplane)
Keep the probe in neutral position while withdrawing or inserting the tip. It can cause esophageal injury if flexed.
We’re not trying to make you cardiac anesthesiologists (they have to know up to 28 views of the TEE!!), so let’s keep it simple. There are 4 main views that we should know as emergency physicians, according to the ACEP Clinical Policies.
Midesophageal Four Chamber View (ME4C)
Midesophageal Long Axis View (MELAX)
Transgastric Short Axis View (TG)
Bicaval View (ME Bicaval)

Midesophageal Four Chamber View (ME4C)
One of the most intuitive, comparable to the TTE’s Apical 4 Chamber View
Can visualize both ventricles and atria as well as the tricuspid and mitral valves in the same plane
Advance the probe to the thoracic esophagus, orient the multiplane at 0-20° in neutral flexion (which is described as keeping the probe straight, neither anteflexed nor retroflexed)
Clinical uses: cardiac activity during pulse check (fine v-fib), evaluating for tamponade, assessment of cardiac chamber sizes, intracardiac thrombus




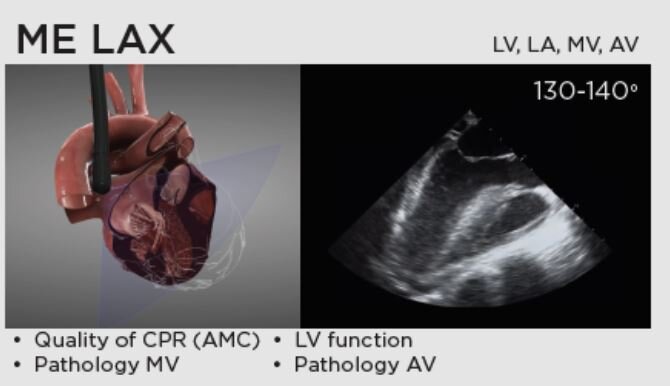
Midesophageal Long Axis View (MELAX)
Compare this with the parasternal long axis view in TTE
You can view the AV valves, left atria and ventricle, and LVOT
Keep the probe in the same position as the MEC4, but increase the plane to 110° to 160° while the probe is neutrally flexed.
Very useful for evaluating the area of maximal compression and effectiveness during chest compressions
Consider adjusting LUCAS device or changes to location if there is evidence of LVOT obstruction tract



Transgastric Short Axis View (TG)
Compare this with the parasternal short axis so you can see all 4 LV walls and the septum
Multiplane should be set to 0°. Probe should be advanced further than previous views and then anteflexed
Cardiac activity, RV size and function can be assessed





Bicaval View (ME Bicaval)
While in the midesophagus, the probe is held in neutral flexion, multiplane at 90-100°.
This is comparable to the IVC view obtained through the subxiphoid view during TTE but with higher resolution, so you are able to see the SVC, IVC, left atrium and right atrium.
In addition to the atrial size and septum bowing, one may evaluate for hypovolemia and guide volume resuscitation.




The Future of TEE
Although still not a common procedure in emergency departments, the future of TEE is endless as it may also be applied to procedural guidance due to the higher quality of image acquisitions. There may be a role for assisting with intra-aortic balloon pumps, ECMO cannulas, TVPs, and REBOAs. Another interesting application may be for TEE- guided resuscitation to take place in pre-hospital settings, taking things one step further (or even earlier to be correct). The MD1 Program, which is a 24/7 physician response vehicle that covers all of New Jersey and is closely affiliated with the RWJBH Newark Beth Israel EMS fellowship program, has been one of the first agencies that has taken TEEs to the pre-hospital settings. A recent case report in 2020 has shown that the TEE saved the life of a patient who suffered a pre-hospital cardiac arrest. Continuous TEE monitoring not only allowed clinicians to adjust CPR hand placement to optimize cardiac output but also identified fine ventricular fibrillation leading to early defibrillation. There has not been any studies that show superior patient outcomes using TEE vs. TTE during resuscitations. However, with the numerous case studies and reports, there remains optimism that with further training and studies, TEEs can become as widely accessible and utilized as the phased array probe we reach for during cardiac arrests.
References
https://www.emsworld.com/article/1223981/md1-response-transesophageal-echocardiography
http://www.emdocs.net/us-probe-transesophageal-echocardiography-in-cardiac-arrest/
https://coreem.net/journal-reviews/ed-tee/
https://www.resuscitativetee.com/protocols
Teran F, Dean AJ, Centeno C, Panebianco NL, Zeidan AJ, Chan W, Abella BS. Evaluation of out-of-hospital cardiac arrest using transesophageal echocardiography in the emergency department. Resuscitation. 2019 Apr;137:140-147. doi: 10.1016/j.resuscitation.2019.02.013. Epub 2019 Feb 16. PMID: 30779977.
https://pie.med.utoronto.ca/TEE/TEE_content/assets/applications/standardViewsHTML5/TEE-HTML5-SV/index.html