
Evaluation of mesenteric adenitis with POCUS in the ED
Written by: Ravneet Kamboj MD, Edited by: Jeff Greco MD.
What is it?
Mesenteric adenitis also known as mesenteric lymphadenitis is a condition that primary presents in children and teenagers however can be seen in all ages.
Symptoms of mesenteric adenitis is usually a self limiting condition that primarily presents with chronic to acute RLQ pain. It involves inflamed lymph nodes in this area.
This inflammation can be caused by viral, bacterial, autoimmune or malignant causes. The most common cause is viral and the most common bacterial agent is Yersinia enterocolitica
Why do we care?
It is important to be aware of for ED physicians because it is known as a “diagnostic mimic” the symptoms, timeline, clinical picture and demographics of mesenteric adenitis closely resembles appendicitis or intussusception
There has been an increasing rate of diagnosis of mesenteric adenitis likely due to increased use of imaging to look for appendicitis. It is often diagnosed on CT scan in the setting of ruling out appendicitis
Studies have shown that WBC and CRP are of limited usefulness in discerning between appendicitis and mesenteric adenitis
The preferred method of diagnosis is by using US, by using ultrasound to evaluate for mesenteric adenitis a person can be spared from the radiation exposure of a CT if a diagnosis can be made. This is particularly relevant since this condition is more common in younger age groups
In one study a full 16% of children being evaluated for appendicitis were found to have mesenteric adenitis after follow through with US, CT or surgery
Evaluation with Ultrasound
Mesenteric lymphadenopathy can often be seen on US. Criteria include seeing 3 or more clustered painful lymph nodes in the RLQ region. A short axis diameter of greater than 5mm is suggestive of mesenteric adenitis
However, there is some dispute about the exact measurement criteria that define this disease process
Some study authors looking at US evaluation of mesenteric adenitis have suggested looking for clustered lymph nodes 10-15mm in the long axis near the base of the mesentery or RUQ is suggestive
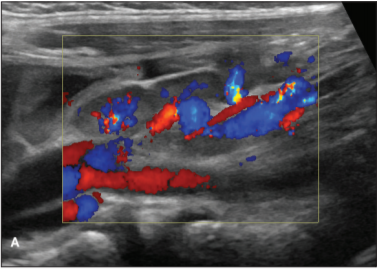
US doppler flow can also be placed over the inflamed lymph nodes which tend to be hypervascular
Some authors believe that if there are signs of mesenteric adenitis clinically, an US showing a normal appendix is enough to rule in mesenteric adenitis even without visualization of inflamed mesenteric lymph nodes
There are often enlarged lymph nodes seen during appendicitis, so visualization of a normal appendix is vital to being able to rule in/out mesenteric adenitis using POCUS
One study by Bourcier et al in the journal of Critical Ultrasound found that out of 158 patients there were 22 cases of lymphadenitis found. Overall the diagnostic accuracy for surgical causes of abdominal pain was 0.89 with the use of US vs 0.70 for diagnoses made with clinical and lab based evaluation only
There are no direct studies measuring the use of POCUS specifically for mesenteric adenitis however numerous studies have validated the sensitivity and specificity of ED POCUS in finding the correct cause of acute abdominal pain.
US technique
The most useful technique for looking for mesenteric adenitis mimics that of looking for acute appendicitis
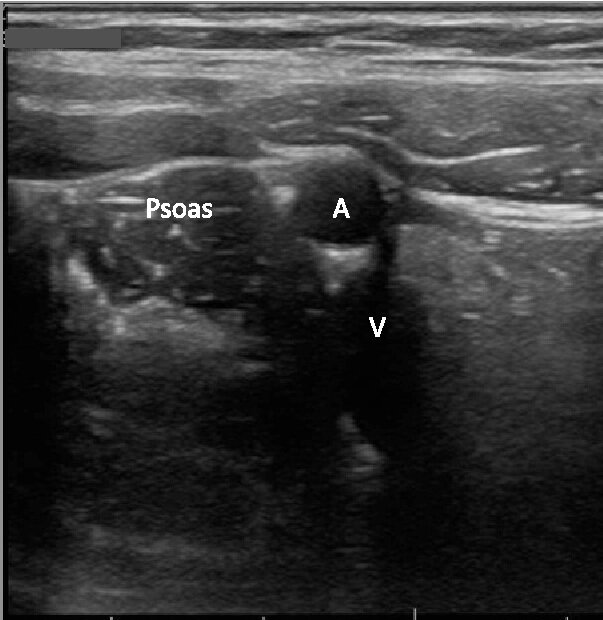
There are several ways of looking for the appendix however one commonly used method is to first visualise the psoas muscle in the RLQ holding the probe in a transverse orientation. You can use a curvilinear probe or even a linear probe on a smaller thinner child
Psoas muscle and Iliac artery and vein seen in transverse orientation
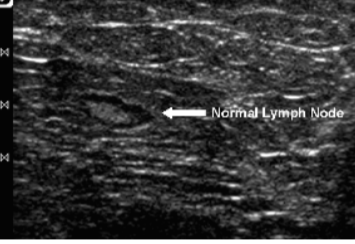
Then scanning in this area in a lawn mower movement should help the operator locate the appendix or see mesenteric lymph nodes, you may run across normal lymph nodes which can be seen below
Lawn mower movement Normal lymph node size and architecture

Enlarged swollen lymph nodes Enlarged Swollen lymph nodes with hypervascularity on doppler

Summary (aka TL;DR)
Mesenteric adenitis can mimic appendicitis/intussusception other causes of abdominal pain in children and young adults
The presence of inflamed hyperechoic lymph nodes in clusters raises the PPV of a patient having mesenteric adenitis vs other pathology
Common values of lymph node size used are greater than 5mm short axis or greater than 10-15mm long axis
Visualizing the appendix has a high specificity for ruling out appendicitis but sensitivity depends on patient and US operator skill
There are other causes of mesenteric lymph node enlargement that should be thought about other than mesenteric adenitis such as giardia, Crohn’s disease, and AIDS.
Seeing lymph nodes that appear “matted”, lack a hilum or are massively enlarged should raise concern and suspicion of other causes like TB or lymphoma
References
[1] Toorenvliet B, Vellekoop A, Bakker R, et al. Clinical differentiation between acute appendicitis and acute mesenteric lymphadenitis in children. Eur J Pediatr Surg 2011; 21:120–123
[2] Sivit CJ, Newman KD, Chandra RS. Visualization of enlarged mesenteric lymph nodes at US examination: clinical significance.Pediatr Radiol 1993; 23:471–475
[3] Thomas Ray Sanchez, MD, Michael T. Corwin, et al. Sonography of Abdominal Pain in Children Appendicitis and Its Common Mimics. J Ultrasound Med 2016; 35:627–635
[4] Bourcier JE, Gallard E, Redonnet JP, et al. Diagnostic performance of abdominal point of care ultrasound performed by an emergency physician in acute right iliac fossa pain. Crit Ultrasound J. 2018;10(1):31. Published 2018 Nov 23. doi:10.1186/s13089-018-0112-5