
Ortho Case: Foot Injury
Author: Jonathan Jong, DO
Editor: Victor Huang, MD, CAQ-SM
Case: A 45-year-old male presents with left foot pain and deformity after he inverted his foot while running on uneven pavement. On examination, the foot is fixed in supination, neurovascularly intact and there are no open skin breaks.
What is the most likely diagnosis, typical mechanism of injury, expected physical exam findings, appropriate imaging modalities, and management plan?


Figure 1. Plain radiograph of the left foot that demonstrate medial subtalar dislocation. Author’s own images.
General
Subtalar dislocation is a rare injury involving the simultaneous disruption of the talo-calcaneal and talo-navicular joints which is supported by strong ligaments and a tight joint capsule [1]. They are classified into medial, lateral, anterior and posterior dislocations based on the displacement of the midfoot [2].
Mechanism of Injury
This usually requires a high energy mechanism like motor vehicle crashes and falls from height. Medial subtalar dislocations are more common and can result from forceful inversion during plantarflexion whereas lateral dislocations occur with eversion [3].
Examination
On examination, subtalar dislocations will present with obvious deformity of the hindfoot and is locked in supination or pronation according to the direction of dislocation [3].
Imaging
Plain radiographs of the foot and ankle should be obtained pre- and post-reduction. It is important to obtain a post-reduction CT scan due to the prevalence of occult injuries including fractures of the fifth metatarsal, the talus, malleolus as well as osteochondral fractures [4,5].
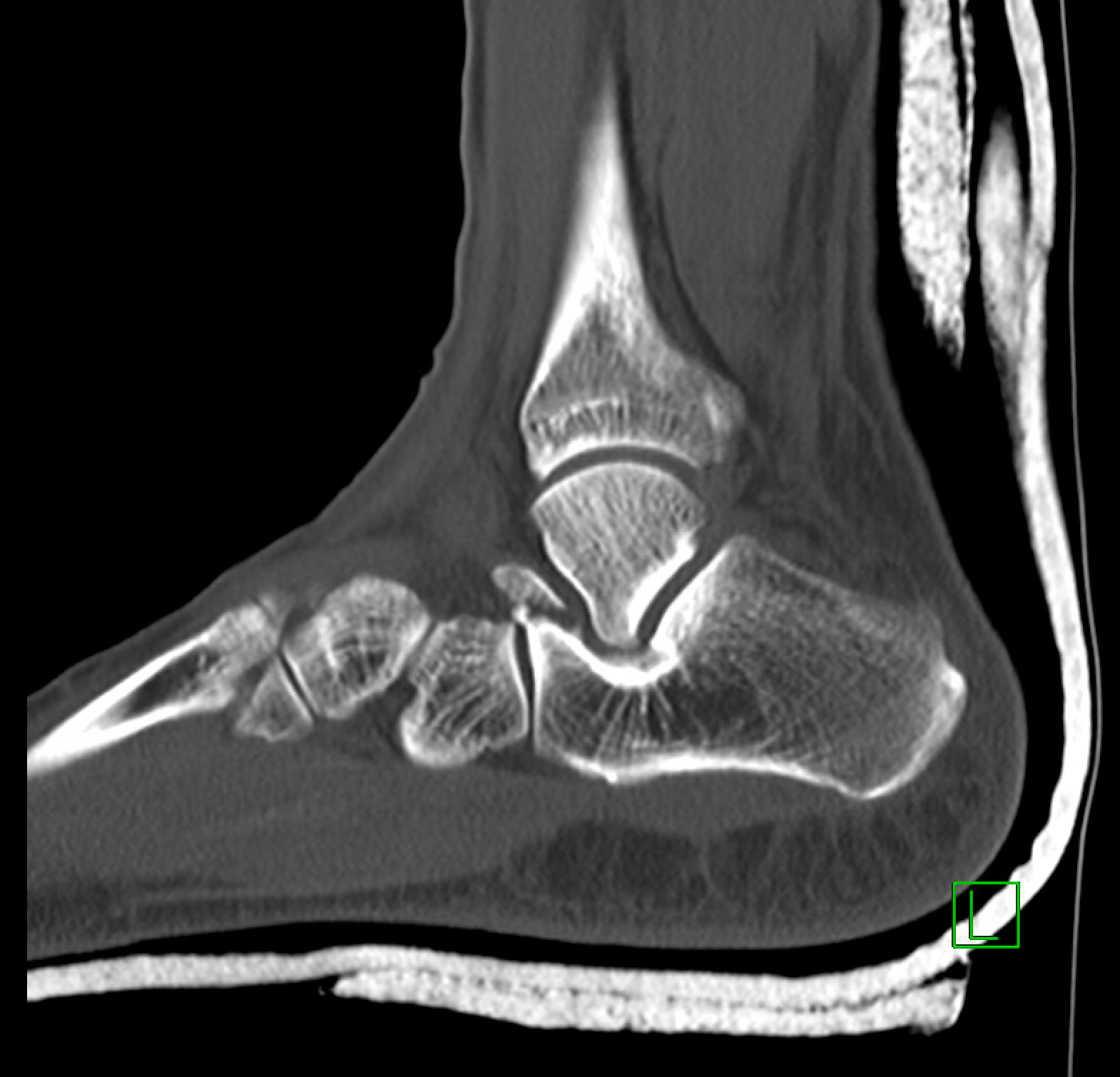

Figure 2. Post-reduction CT images that demonstrates a fracture of the anterior process of calcaneus and interval reduction of subtalar dislocation. Author’s own images.
Management
These patients should undergo closed reduction that often requires procedural sedation [7]. Patients should be positioned with their knee flexed to 90 degrees in order to relax the gastrocnemius and soleus muscles. Reduction can then be performed with traction and countertraction, accentuating the deformity and then reversing the mechanism. Immobilization can be achieved with placement of a short leg AO splint and made non-weight bearing [5,6].
Orthopedics should be consulted for open fractures, neurovascular compromise, and irreducible dislocations due to interposed soft-tissue blocking reduction [3,5].
References
DeLee JC, Curtis R. Subtalar dislocation of the foot. J Bone Joint Surg Am. 1982;64:433-437.
Bibbo C, Anderson RB, Davis WH. Injury Characteristics and the Clinical Outcome of Subtalar Dislocations: A Clinical and Radiographic Analysis of 25 Cases. Foot & Ankle International. 2003;24(2):158-163. PMID: 12627624
Giannoulis D, Papadopoulos DV, Lykissas MG, Koulouvaris P, Gkiatas I, Mavrodontidis A. Subtalar dislocation without associated fractures: Case report and review of literature. World J Orthop 2015; 6(3): 374-379. PMID: 25893182
Bibbo C, Lin SS, Abidi N, Berberian W, Grossman M, Gebauer G, Behrens FF. Missed and associated injuries after subtalar dislocation: the role of CT. Foot Ankle Int. 2001 Apr;22(4):324-8. PMID: 11354446
Perugia D, Basile A, Massoni C, Gumina S, Rossi F, Ferretti A. Conservative treatment of subtalar dislocations. Int Orthop 2002; 26: 56–60. PMID: 11954852
Lasanianos, N.G., Lyras, D.N., Mouzopoulos, G. et al. Early mobilization after uncomplicated medial subtalar dislocation provides successful functional results. J Orthopaed Traumatol 12, 37–43 (2011). PMID: 21308390
de Palma L, Santucci A, Marinelli M, Borgogno E, Catalani A. Clinical outcome of closed isolated subtalar dislocations. Arch Orthop Trauma Surg. 2008 Jun;128(6):593-8. PMID: 17909825