
Duck, Duck, Goose (Using POCUS for ETT placement confirmation)
Written by: Tina Yang, DO. Edited by Jeff Greco, MD
In patients undergoing tracheal intubation, there is currently no universally accepted gold-standard to confirm the location of the endotracheal tube (ETT). Many methods are utilized and are often used in combination with each other. Each confirmation modality has their potential benefits and limitations. Chest x-ray may take a long time to confirm, as well as exposes the patient to additional radiation and adding to their cost of treatment. Chest auscultation can be inaccurate or difficult especially in loud environments. End-tidal carbon dioxide (CO2) detection is often regarded as the best confirmatory test, however, it has been shown to have an error rate as high as 1/10 for proper determination of ETT and is shown to be only 65-68% sensitive in detecting the correct ETT location during cardiac arrest. The lack of a single, reliable test to confirm ETT placement can potentially lead to confusion regarding the location of the tube. This confusion can result in both unrecognized esophageal intubations, as well as successful tracheal intubations that are subsequently removed, subjecting the patient to further unnecessary attempts at airway management.
Ultrasound can provide a rapid evaluation to confirm proper endotracheal tube placement, with fewer complications. An article by Gottlieb, et al. called Ultrasonography for the Confirmation of Endotracheal Tube Intubation: A Systematic Review and Meta-analysis found transtracheal ultrasonography was 98.7% sensitive (95% confidence interval 97.8% to 99.2%) and 97.1% specific (95% confidence interval 92.4% to 99.0%) with a positive likelihood ratio of 34.4 and a negative likelihood ratio of 0.01. The mean time to confirmation was just 13 seconds.
Technique:
Place the linear ultrasound probe just superior to the suprasternal notch. This should be a transverse view anterior and over the trachea.

Figure 1. Transverse placement of the high-frequency linear transducer over the trachea just cephalad to the suprasternal notch. Image courtesy of Werner et al.
Ways to confirm placement:
Video 1: Dynamic (real-time, concurrent with laryngoscopy and ETT placement) video showing successful tracheal placement of ETT.

Video 2. Dynamic video showing placement of ETT into the esophagus (located in left paratracheal location in approx. 70% humans).
One air-mucosal interface = tracheal intubation

Two air-mucosal interfaces = esophageal intubation

“Bullet sign”= tracheal intubation
Reverberations are seen in the anterior portion of the lumen of the trachea, just posterior (or deep) to the anterior wall.
Image from Favot M, ALiEM 2015: Ultrasound for Verification of ETT

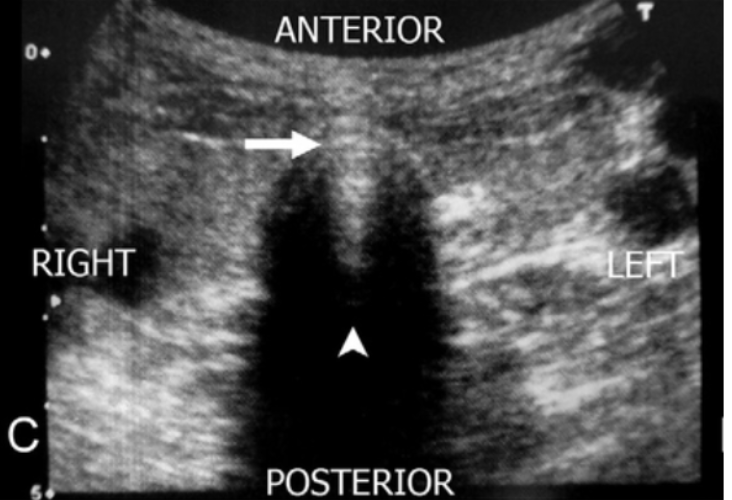
“Double track sign” = esophageal intubation
Image from Favot M, ALiEM 2015: Ultrasound for Verification of ETT

Snowstorm sign” = tracheal intubation (transverse view)
Image from Patil V, JECCM 2019: Utility of ultrasound of upper airway for confirmation of endotracheal intubation and confirmation of the endotracheal tube position in the intensive care unit patients
Limitations
Training and sonographer experience is an important factor for using POCUS
POCUS should not be used for every intubation confirmation.
Space is tight and there may not be room for the ultrasound machine
Transducer on the trachea may make intubation more difficult
When it is not feasible to use POCUS for ETT confirmation:
Large neck masses
Abnormal upper airway anatomy
Soft tissue air
Cervical collars
Significant neck edema
Conclusion
Confirmation of ETT placement with POCUS should be used in conjunction with other confirmatory methods such as but not limited to the following: chest and epigastric auscultation, end-tidal capnography, ETT condensation, visualization of chest expansion, clinical improvement, and chest x-ray, as no one singular method is perfect. POCUS is a powerful tool when used in the hands of an experienced and well-trained sonographer. Judicious use is required since it is not always appropriate for all intubations and should not become an obstacle in placing an ETT.
References
American College of Emergency Physicians Board of Directors. Verification of Endotracheal Tube Placement. policy statement. Revised April 2009.
Tanigawa K, Takeda T, Goto E, Tanaka K. The efficacy of esophageal detector devices in verifying tracheal tube placement: a randomized cross-over study of out-of-hospital cardiac arrest patients. Anesth Analg. 2001 Feb.
Li J. Capnography alone is imperfect for endotracheal tube placement confirmation during emergency intubation. J Emerg Med. 2001;20(3):223-229.
Werner S, Smith C, Goldstein J, Jones R, Cydulka R. Pilot study to evaluate the accuracy of ultrasonography in confirming endotracheal tube placement. Ann Emerg Med. 2007;49(1):75-80.
Gottlieb M,et al. Ultrasonography for the Confirmation of Endotracheal Tube Intubation: A Systematic Review and Meta-Analysis. Ann Emerg Med. 2018. PMID: 30119943
Mark Ramzy, DO, "POCUS for Endotracheal Tube Confirmation", REBEL EM blog, January 31, 2019. Available at: https://rebelem.com/pocus-for-endotracheal-tube-confirmation/.
Favot M, Ultrasound for Verification of Endotracheal Tube Location. ALiEM. Link Here
Abbasi S, et al. Direct ultrasound methods. European Journal of Emergency Medicine. 2015. PMID: 24441884
Chou E, et al. (2011). Tracheal rapid ultrasound exam (TRUE) for confirming endotracheal tube placement during emergency intubation. Resuscitation. 82. 1279-84. 10.1016/j.resuscitation.2011.05.016.